Advancements in digital technologies and materials in recent years have been very attractive by allowing us to implement a digital workflow when treating our patients, which is less labour intensive and more interactive. In this article I explore the differences between the different technologies, and whether an end-to-end fully digital workflow can be used for the production of Immediate Final Teeth™ after surgery (using milled PMMA over a titanium frame) and ultimately replace the human touch when using individually set acrylic teeth over a titanium frame.
Background
Our current protocol has changed to an almost fully digital workflow over the last 5 years.
It started with the introduction of a technology to dentistry called photogrammetry, which for many years before has been used in the aeronautical and automotive industries for replicating parts due to its high precision and accuracy. It is a method scientifically proven for its accuracy, and widely used in other industries. The technology was adapted to Dentistry by a Spanish engineer, Adrian Hernandez, who saw his father receive dental implants treatment and realised that clinicians had real struggles to produce passively-fitting full arch restorations on implants.
Adrian developed the PIC camera, a sophisticated but amazingly simple hand held capturing device, which uses photogrammetry to determine the precise positions and inter-relationship of dental implants to each other.
Over the last 10 years dentistry also saw significant advancements in another digital impression technology, the intra-oral scanner. This technology has been successfully used for taking digital impressions of natural teeth and single implants, but precision in full-arch implant restorations has always been a challenge. This is because these technologies rely on stitching of videos or images. Inherently, the more stitches that are required the higher the distortion. So if an impression is required of one, two or three teeth, and the interrelationship of those teeth to each other is not an absolute priority, then the technology is ideal, and as a result digital scanning has emerged as a routine technique for that purpose.
However, when doing full arch restorations the impression is not only longer but it also changes direction with the curvature of the arch. This is where technologies that rely on stitching have fallen apart, especially when it comes to dental implants, which are ankylosed in the bone and cannot absorb discrepancies or a misfit (unlike teeth that can absorb a misfit due to the presence of a periodontal ligament).
It is kind of similar to using your iPhone to take a panoramic image. The longer the panorama, the more distorted the horizon becomes. This is a known scientific phenomenon. The distortion becomes even more significant when changing direction, such as when attempting to take a digital impression of a full arch. Whereas with photogrammetry, the spread of implants and horseshoe form of an arch are actually advantageous in making the impression precise.
Until the advent of PIC, there was no accurate option for implant impressions other than using our standard impression technique, which really stalled our desire to move to a digital workflow.
With the arrival of PIC we were able to change to a digital workflow that would produce absolute accuracy in the digitised representation of the implant positions.
Our workflow involves using the PIC camera to capture the implant positions, correlate them to the original teeth through a mid-scan done during surgery using an intra-oral scanner while retaining certain elements (such as teeth or a denture) that can enable such correlation, and which in turn can be correlated to the digital smile design. A lack of absolute accuracy of the intra-oral scanner is not so much of an issue for the mid-scan or soft tissue (because of the compressible nature of soft tissues and its ability to accommodate discrepancies). It is then correlated to the absolute accurate scan of the implant positions.
All the digitised models are then sent to the design centre. The laboratory finalises the design using the mid-scan, the post operative scan and the precisice implant capture and shares this with the dentist, who uses a simple and relatively inexpensive 3-D printer to produce templates of teeth that represent the digital design. These templates are fitted on the implants only within 2-3 hours (on the same day), and they are used to determine final Occlusal Vertical Position and to fine tune the aesthetic, function etc. before proceeding with production of the final teeth.
We then take pictures of the templates in the mouth as a reference for the technician. By the time this is done, the local anaesthetic has worn off somewhat, so the patient is able to smile and make expressions when assessing the smile. Importantly the swelling has not as yet set in so it is the best time to verify the aesthetic aims for final smile design.
The adjusted templates and the confirmed bite are then either scanned again or removed from the mouth and sent to the lab (along with the bite registration) for production. Whilst all this is happening, the digitised version of the prosthetic design enables the laboratory to design the titanium bar for the final teeth and even to commence the milling process while the templates are on their way to the lab.
Another set of templates can be printed and can be worn by the patient immediately after surgery for up to a week until the final teeth are produced.
Once the templates arrive in the laboratory and the milled bar is ready, the technician commences the process of setting acrylic teeth on top of the titanium bar and their individualisation. The technician used the photographic references to fine-tune the aesthetics and to individualise the prosthesis according to the dentists and patient's desires.
High pressure acrylic injection moulding is then used to set the teeth in high impact acrylic. The final teeth are ready to be inserted typically within 24 hours, or sometimes up to 5 days depending on the clinic location.
What are the problems and why explore alternatives?
The digital workflow described above has produced outstanding results in terms of aesthetics, function, comfort and precision fit. However there are still some areas where improvement could be sought:
Problem 1: The Immediate Final Teeth have a breakage rate of 1 in 8 (we tell patients 1 in 6) over a 5 years period. Breakages are a significant inconvenience for the patient as well as for the practice, especially when the laboratory is interstate and this involves substantial transportation costs to and from the lab for a quick delivery.
Problem 2: The PIC Camera is not accessible or affordable by every practice. It would be advantageous if digital scanning technique which are already being used by most practices for multiple other uses can also be utilised to obtain an accurate impression of the implants. The question is, are we there yet (or will we ever be) with scanners that rely on stitching?
What is the proposed solution?
Overcoming Breakages
It has been proposed that the issue of breakages can be overcome by using a milled PMMA material over the titanium frame, and if the PMMA discolours or breaks, it can be replaced with Zirconia possibly even on the same frame.
More Accessible Technology with Similar Accuracy
It is proposed that distortion from stitching can be overcome by using longer and triangular scan bodies.

Both proposals are a part of a system used by a state-of-the art milling facility, Osteon Medical, whose production system relies on fully-digitised workflow. It allows the dentist to share the data with a lab in a remote location, and vice versa, and to use cost-effective printers to print the templates on site at the clinic. I have recently participated in the use of this system on 6 arches (4 patients) and have mostly positive feedback, though the critical factor that I was still unable to verify was precision fit, and the durability of PMMA compared to High Impact Acrylic.
Discussion
The tremendous improvement to the design of the scan bodies making them longer and triangular (Battle Ships Scan Bodies, "BSSB") goes a long way to improve accuracy. Below is my experience and some ongoing concerns:
HANDELING & PRECISION FIT
- The scanning system of the battle ships is not as fiddly as I expected. They were large and easy to handle. The process takes slightly longer than PIC, but acceptable. I especially like the metallic collars/interfaces with give a great feel of the fit (compared to the PIC flags which are a ‘softer’ feel).
- One scan is taken left to right and another seperate scan is taken right to left. The two scans are done in order to verify that the scans match and are accurate, and if there is a mismatch the entire scan is rejected. In two out of the six arches that I observed there was an issue and the scans were rejected requiring new double-scans. This is not ideal because the patient is already awake by the time the discrepancy is picked up and the scanning is more difficult and uncomfortable. The fact that there is a safety net with the second scan for verification is reassuring in relation to fit of the final bar, but this also confirms that there are still issues with this scanning method requiring this kind of verification. I am conscious that the images are still stitched and therefore the accuracy can never be as predictable as using photogrammetry or physical impressions with copings and a luted bar. However using this system and putting aside the inconvenience of having to do another scan if the first is rejected, when a scan is accepted there is a level of certainty in relation to the fit of the final bridge.
- The printed templates were not completely passive (different to what we get when using PIC which has always been passive except when there was an operator error). This can be due to the printer and cleaning or curing of the printed templates or the access channels, or it may have been the discrepancy in the BSSB scan that was subsequently picked up. This is not too much of a concern since the templates are only in the mouth for less than a week, as long as the final bar is passive.
- The laboratory design process and correlation of the digital design to the scanned implants is too long (over 3 hours)! This meant that some patients were not able to get their templates produced on the same day. This is not ideaI as there is more swelling in the next day and it is impossible to make an assessment of the templates as to the adjustments required to the original design for the final aesthetics.
- I liked the fact system can be used with any intra-oral scanner that exists in the practice. This is cheaper and more practical that buying or transporting PIC between locations.
PRODUCTION
The Milled Titanium Frame
The quality of milled Titanium frame produce by the laboratory using industrial systems is second to none. The collars and screw channels are machined and as good as I have seen. The fact that a titanium frame is used to support the teeth is critical, and key to enable the implants to work in a group and offer a protective mechanism during healing.
Milled PMMA
Most of my concerns in relation to using this material are alleviated as long as this is supported by a titanium frame.
The PMMA is milled according to the digital design over the titanium frame, and the gum colour is added on top. As such it is easier, quicker, much cheaper to produce and well suited to replicating a purely digital design and workflow, however:
The tensile strength of a milled PMMA has typically been inferior to the tensile strength of the Heraeus teeth that we have been using. Newer PMMA materials have comparable strength, but the unlike individually set Heraeus teeth, the PMMA is a monoblock which means that the teeth are connected to each other. This reduced the amount of flexture of individual teeth and improves durability, albeit at a slight compromise in the aesthetics.
Since the PMMA sleeve is printed over a bar, the finished base is often necessarily wider at the gum interface to avoid chipping of the edges, which is not ideal for cleanability. The design can be improved (as long as the implants are well placed), and I have seen instances when this has been as good as it needs to be.
The underside of the titanium frame is finished short to allow for a wrap around of the PMMA sleeve restoration. The gap is filled with powder-liquid acrylic. This has the advantage of allowing for relining of the bridge in the future if necessary, however the bonding of the two materials and the seal long term is somewhat of an unknown.
Adjustments are not simple – adjusting the contours strips the colour and this needs to be reapplied which can be fiddly. If more substantial adjustments are required the entire bridge would need to be remade, which is cheap enough to do.
A purely digital design lacks the human touch. Although some amendments can be made digitally, this is still inferior to hand-made arrangement of teeth.
The aesthetics are great in pictures, but inferior to Acrylic in real life on close up. Whilst it is possible and simple (using digital records) to convert this to Zirconia teeth, there is an issue in double arch cases with Zirconia against Zirconia, and generally in our protocol we recommend for one arch should remain in Acrylic or PMMA.
Unfortunately I was not able to see the final milled PMMA on the bar for the six cases that I observed due to courier delays. I saw pictures of the interfaces being more hygienic, which was great but I still need to evaluate this in person. It also needs to be seen after 3 and 5 years in function in order to be able to compare the performance of PMMA over time in terms of both durability and aesthetics.
Turnaround
The process is adequate as long as it is inserted within a week because the healing implants are most vulnerable in weeks 2-4.
Opinion
Technicians are often what makes us dentists look great, but just like us they are notorious for dipping into technologies and materials that they find easier or fascinating. Brilliant as our technicians might be as artists and fabricators, what they lack is a deeper level of understanding of the clinical/biological nature of what we do. They are not trained to fully understand the differences between Tooth-born VS Implant-born restorations.
We should be making clinical decisions based on science and in vivo experience not based on a trend of attractive which we might find fascinating at any one time.
It is the dentists role to instruct the technician in relation to a clinical protocol not the other way around, because ultimately the responsibility and risk (including the surgical and long term risks) remain with the dentist and not the technician.
What the BSSB scanning system lacks right now is a confirmation of the accuracy of this method. The scanning technology is known to be inaccurate, but the use of the BSSB (if proven) could well be an answer to the PIC technology.
For the Nexus/Osteon system I have suggested the following:
- introduction of instant verification of scan accuracy to avoid having to do a re-scan when the patient is awake
- a booking system to ensure a CAD technician is available to correlate the scans to the design and output for printing within 1-2 hours
- quicker production time and transport ideally for insertion within 2-3 days
- verification of accuracy of the scanning of BSSB. There is highly likely to be a level of inaccuracy, but the safeguard of second scan verification would be adequate provided that any mismatch can be instantly verified
- verification of the performance of PMMA over time in terms of aesthetics and durability
- a system to deal with any required/requested changes after insertion
- for Nexus, an open system platform to allow design and production by any laboratory the dentist trusts and for any kind of restoration he/she prefers
Until such time that we have a comparative study of the accuracy of BSSB, and more data about the performance of PMMA, I am cautiously optimistic about the use of BSSB and PMMA. I am personally still in favour of PIC impressions (I have no commercial interest whatsoever in this) and the Immediate Final Teeth system with milled bar and Acrylic Teeth. We have done thousands of cases to date, some are over 15 years old and still look great and don’t need to upgrade, so we know what to expect! My laboratory (as most similar laboratories) can also produce PMMA on milled bars, but I am still simply not convinced. With our 1 in 8 breakage rate this is not enough (for me at least) to change to something that is currently still an unknown.
It is also noteworthy that management of breakages has become far less inconvenient with access to 3-D printing. It is now possible to replace the broken prosthesis with printed teeth and send the broken one for a repair +/- upgrade! Upgrades to zirconia are only done based on indication, often upgrading only one of the arches to Zirconia not both. The acrylic setting has the kind of impact absorption that is more favourable (because the implants themselves are ankylosed) compared to Zirconia.
More importantly, when a breakage does occur, we can use the pattern of the breakage as a clue to diagnose bigger issues. It is a circuit breaker and allows us to address the causes and not just the problem.
Disclaimer: I do have the benefit of having an in-house laboratory and access to multiple PIC systems, whereas for the vast majority of dental clinics using BSSB and PMMA could be a more accessible and cheaper alternative.
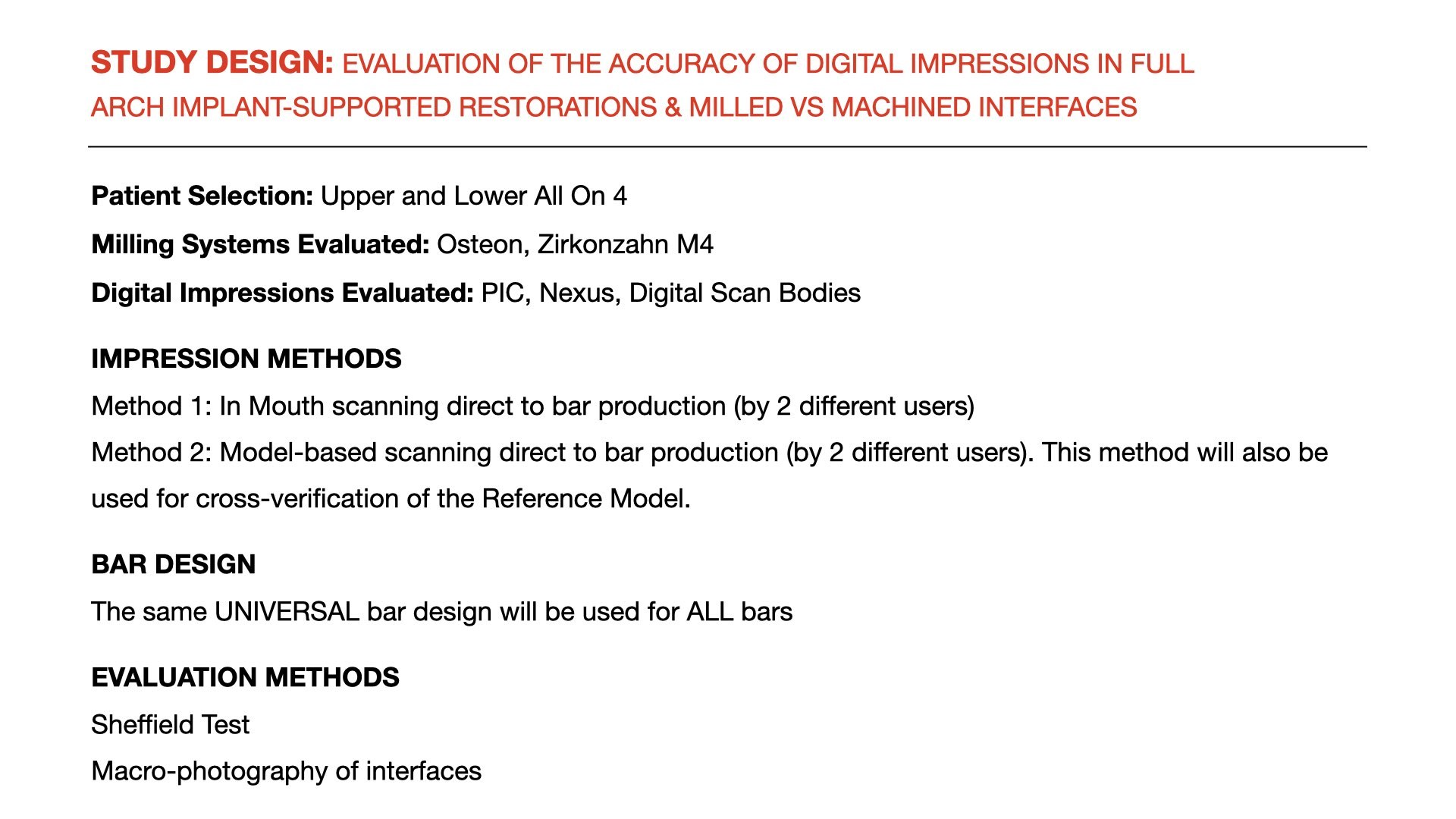
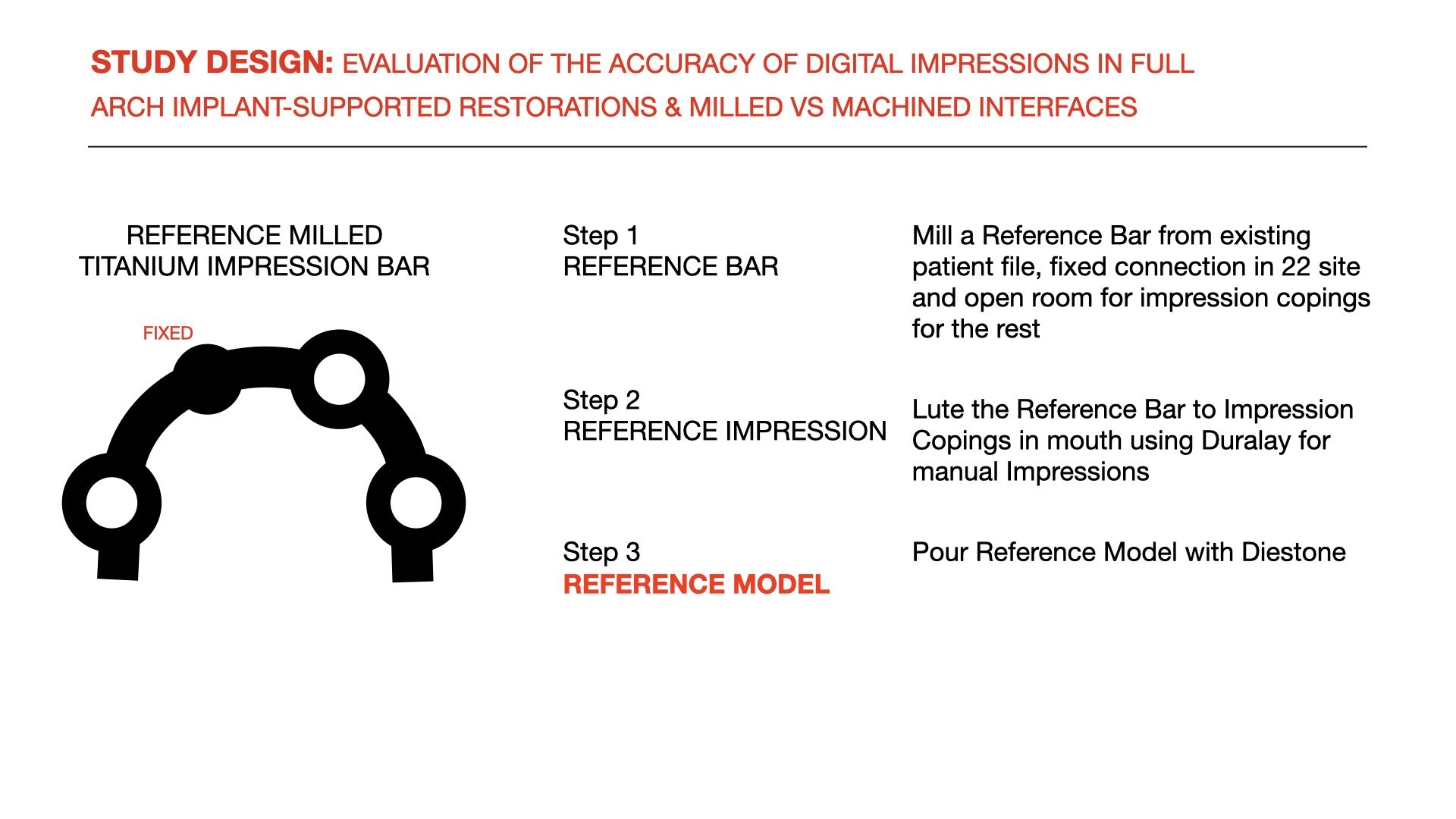
STUDY PROPOSAL
It would be useful to do a comparative study to confirm that using BSSB along with standard scanning systems (like Trios) can produce results as accurate as photogrammetry (which is already scientifically proven, albeit in other industries). This would enable clinicians who don't have access to an expensive digital camera like PIC to use their existing intra-oral scanners to obtain accurate impressions. Such a study would improve confidence in a system which still to a large degree still relies on digital stitching which has known distortions. I approached Osteon Medical and proposed to undertake a study to compare the different scanning methods as well as the quality of bars with Osteons state-of-the-art industrial milling machines compared to more broadly used office-based milling systems. Osteon have declined the in-mouth method but will consider the in-vitro method.
I will update this blog with the outcome.