
New Methods for Preservation of Bone in Full Arch Implant Cases
Regeneration and preservation of jawbone has been an area of great interest for as long as dental implants have been around. Many techniques have been described in the literature including using autografts, allografts, xenograft, in block or particulate forms, all kinds of bones substitutes to regenerate bone that is lost with the loss of teeth.
Regeneration and preservation of jawbone has been an area of great interest for as long as dental implants have been around. Many techniques have been described in the literature including using autografts, allografts, xenograft, in block or particulate forms, all kinds of bones substitutes to regenerate bone that is lost with the loss of teeth.
We have long known that alveolar bone is bundle bone, the existence of which depends on the periodontal ligament when teeth are present, so a newer hypothesis emerged that if we can preserve the periodontal ligament then we can also prevent resorption of bone. To preserve the ligament the tooth is only partially extracted with the superficial parts of the root only remaining and the rest is removed when drilling to insert the implant. This is referred to as PET (Partial Extration Therapy).
I have some minor reservations regarding this technique, including:
A lack of vascularisation …the part of the implant that is in contact with an avascular piece of the tooth has no blood supply or clot forming a biological seal
Implant integration requires rigid ankylosis, so this concept doesn’t mix well with the required functional micro-movement to stimulate and preserve the bundle bone through the periodontal ligament.
However, these things alone might be proven in the literature over time through a healing mechanism that we may still not be fully understood at this time.
My main issue with this is not so much the actual biology, or technical difficulties with PET, but the fact that despite there being evidence of horizontal preservation of bone, in the cases that I have seen there has not been a predictable retention or regeneration of the papilla, especially in full arch cases, and the restorative space is compromised because of the shallow placement of the implants. The result can be devastating for patients when dark margins or black triangles exist’ like pictured here.
Also the lack of restorative space leads to a limitation in our ability to design an ideal restoration and in turn compromises in comfort and durability, as well as impaired hygiene.
When a colleague posted a nice case of full arch using the PET technique, I was invited for comment.
Below is my discussion with my various colleagues, some of which are involved in the PET research:
Colleague 1
Why Don’t you try this ??
My Reply
This is a very nice presentation, but to answer your question, the reason I don’t do this today is predominantly because there are no convincing studies as well as personal experience with similar methods many years ago.
There are also numerous other ways to preserve or regenerate sockets, which I have used over the years, and which do not present an added risk of sequestration or infection. My aim with all these methods is to achieve aesthetic gingival choreography.
What I found was that the most important factors to achieve this were the presence of adjacent natural teeth and avoidance of adjacent implants. Also important is sealing the sockets with an anatomical immediate restoration and respecting the biological nature of healing and remodeling, in particular the requisite vascularisation at the implant interface.
When it comes to full arch restorations it is difficult to achieve papillae and high aesthetics using preservation or regenerative methods. Not impossible, but very difficult and costly, …and very much subject to changes over time, such as development of black triangles having to add some “pink” to the restoration, which in turn impairs hygiene.


Apart from that, there is the loss of the bundle bone over time, which can lead to recession followed by food impaction beyond the curving contours at the cervical, as well as a loss of lip support. Exactly what are evidently the problems above (one of the cases of Colleague 3).
These procedures that we do are great to test our surgical and restorative skills. Though beautiful as these techniques can be, as so expertly demonstrated here, my concerns today are to do with long term hygiene, comfort and durability due to a lack of restorative space in other cases using similar techniques.
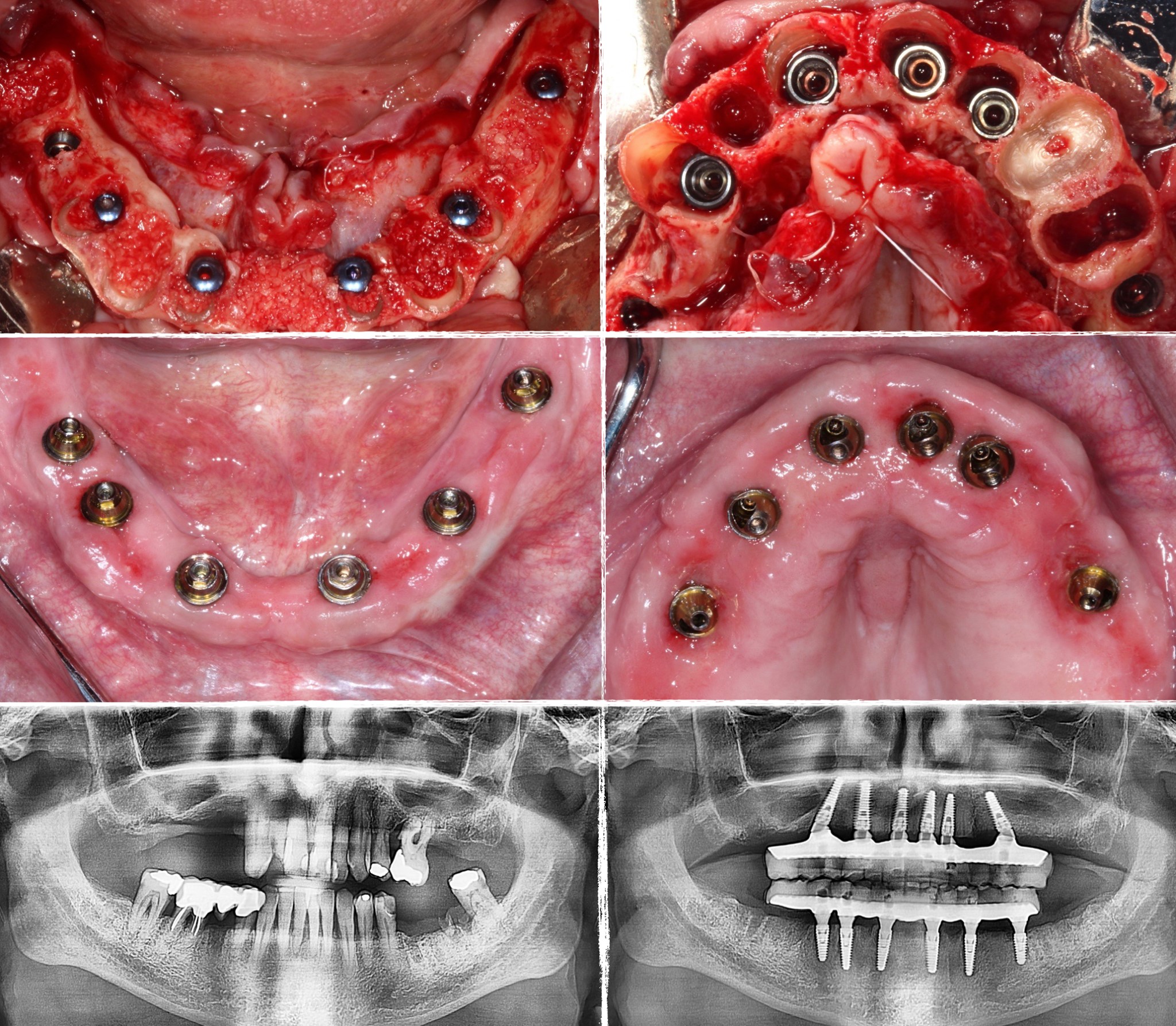
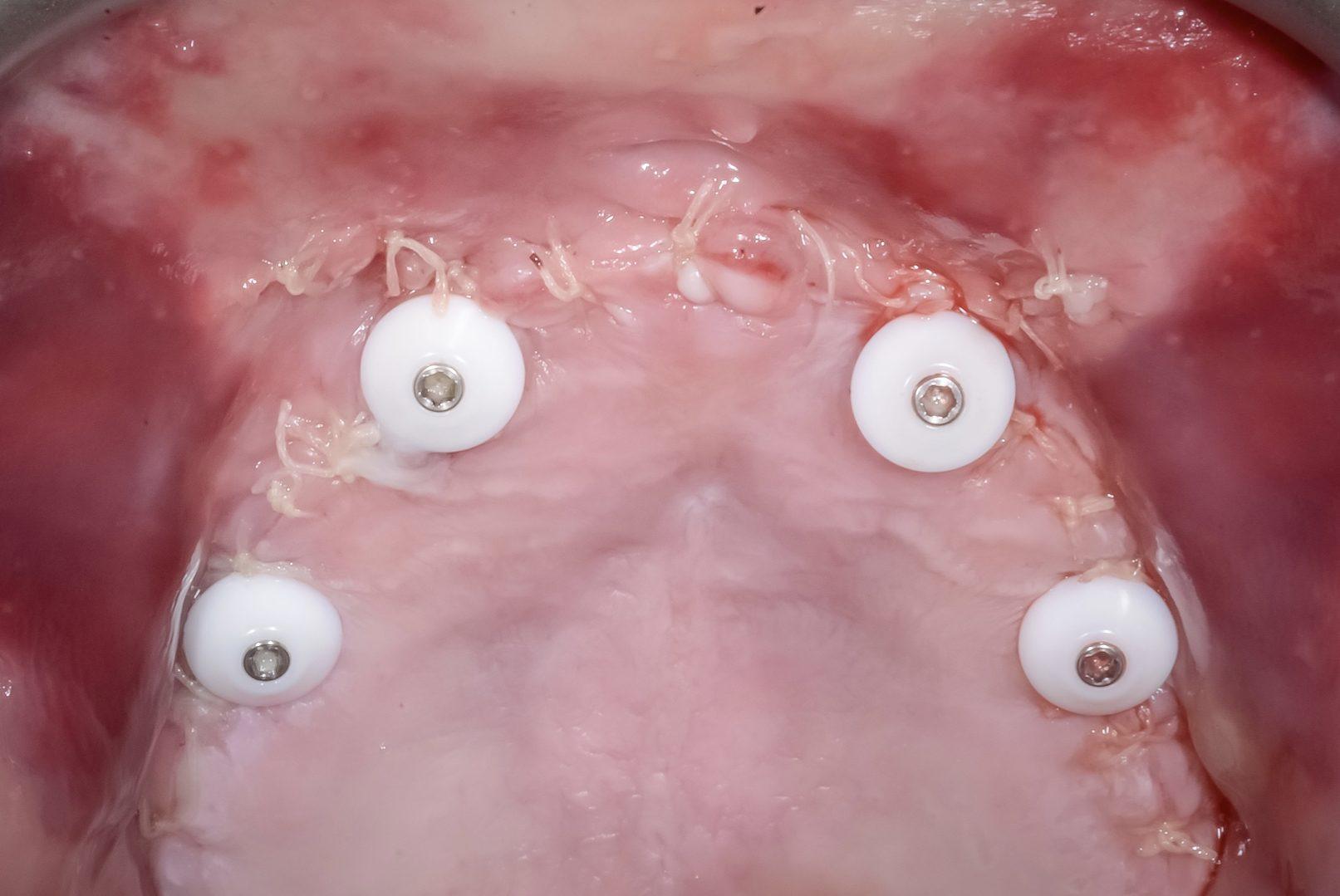
Today my focus is on consistently being able to achieve successful long term results, and to that effect I have to consider the important opportunity that may be present (before positioning any hardware) to prosthetically recreate beautiful, hygienic and stable gums when planning a full arch restoration. Hygiene and comfort are also improved with a flat interface and using only four implants unless otherwise dictated by biomechanical considerations.
Different strokes for different folk, … nice work!
Colleague 1
No convincing evidence of PET? Have you not seen 10 years of scientific literature on PET?
My Reply
No. There is literature on hundreds of types pf techniques, it doesn’t mean they are convincing, or the we should be using all the techniques. There is more to success than osseointegration, and nothing like experience to teach us.
Colleague 2
This Is a new procedure and obviously requires a debate and more clinical evidence. So, some questions for you:
– Infection Is a very low risk, why?
– What chance to maintain papilla between 2 implants on convention al method?
– What Will bè the fate of bundle bone with any other technique?
– Any other technique providing so beautiful result, single step procedure, and no additional surgery cost and waiting time?
New approach requires a new vision sometime. I Will be glad to share some clinical observation Just to promote more discussione on this field between us.
My Reply
Well said and I agree, but for me having done similar procedures many years ago, the papilla loss, restorative space issues and hygiene issues are things that I have learnt through experience. Also cost and complex process for the patient.
Colleague 3 (PET Researcher)
It is perfectly fine if you are not comfortable with the necessary effort to provide PET for your patients. However, please do not deny the evidence that exists to validate this approach. I have been placing implants and critically observing and documenting outcomes more than 30 years. The most recent 5 years have included PET. Both I and my patients can clearly see and understand the difference and prefer PET.
Hey I have little desire to perform Zygomatic implants on my patients, but I am sure there are Patients who want this type of treatment.
My Reply
As much as I admire your research, I don’t agree with your comment on effort. My efforts as to advanced techniques have with time and experience turned into an effort towards a system which achieves predictable results for a lower cost and higher patient satisfaction.
From the caliber of dentists and specialists that I am fortunate enough to meet at my residencies or conferences, the issues that I have mentioned in my initial reply are global, and I am acutely aware that the number of experienced clinicians who recognise the difference and move away from preservation and/or regeneration in full arch case planning is growing fast.
With all due respect I don’t agree with your approach, especially for full arch reconstruction …it all depends on whether the focus is on a technique VS the result.
Like I said, different strokes for different folk, and I do congratulate you on your achievements and hope to meet and compare notes one day.
Colleague 1
Why don’t you post some of yours cases so we can compare ?
My Reply





Final Word…
Like with many other things, in the right hands, for the right patient and the right indication PET can certainly be considered in an attempt to preserve bone when replacing a single tooth. Unfortunately it does nothing to preserve or regenerate papillae or result in an aesthetic gingival choreography in full arch cases, or even cases that present with already compromised gingival aesthetics.
Teeth are extracted due to disease, trauma, function and/or aesthetics. They are rarely extracted due to health. As such the preservation of the any portion of the root in the absence of health or other ideal parameters goes against the laws of nature, and will be more susceptible to some kind of compromise.
Experience teaches us that we really should respect nature, and nature tells us that when a tooth is lost the bone and papillae go with it. It then follows that if an ideal gingival choreography cannot be predictably regenerated in full arch cases even with PET, our focus should shift to predictably recreating it by adjusting our technique, otherwise we run the risk of missing this opportunity and our patients ending up with restorative, aesthetic, functional and hygiene issues that become far more difficult to fix.
Many of the referrals that I get today for revision surgery are to do with the my colleagues best intentions of following the idea of conservation and preservation with full arch implant therapy, which end up being problematic in more ways than one.
A definitive approach is the most conservative approach.
As we speak, here is a fb message I just received only days ago from a patient who had that kind of approach back in 2003. In a private message she told me her teeth look as good today as they looked when I first put them in.



Reply by Master Dental Technician:
Looking back at over 40 years of experience in the dental technology industry i have to agree with you Alex.
As you said there are many ways to skin a cat.
However maintaining the architecture of the soft tissue and specifically the papilla is the problem.
I have seen to many cases over the years that were failing after a short time.
As a laboratory owner who makes the restorations I do not want them to turn into permanent repairs or remakes.
Only when I met you some 7 years ago and looked at how you had changed the way these cases where done, I got interested again.
It all started with you explaining to me that the space made the case.
It made a lot of sense.



{kind=link}