
Removal of Teeth, Bone Atrophy & Preservation (or Loss) of Bone with Dental Implants
Removal of teeth is something that is very difficult for us as dentists to recommend, and we battle with this every day. When the outlook for the teeth is not great, I often emphasise that a better result can be achieved by addressing things early before the further spread of disease and destruction of bone.
Some of the questions put to me by a colleague on facebook are to do with the effect of tooth removal on bone atrophy…
Question 1: When you remove all of a patients teeth to place 4 implants- how do you stop continued bone atrophy?
My Reply
There are 2 kinds of atrophy:
- Natural Atrophy
- Iatrogenic Atrophy
NATURAL ATROPHY
Atrophy of the alveolar bone (which is supported by teeth …when healthy) is a natural process that occurs as a result of tooth loss. This cannot be stopped.
There are various techniques to regenerate bone, but when multiple teeth are lost the most challenging part is the papillas, and the subsequent maintenance of prosthetic solutions to the compromised papillas.
IATROGENIC ATROPHY
Bone atrophy is also exacerbated by fitting of dentures, and also in cases of “supervised neglect” when we do not (or cannot) adequately address tooth-related disease processes that cause further bone destruction. It can also be iatrogenicslly caused by poor implant placement, poor prosthetic solutions, biomechanical factors, etc.
All-On-4 is only one treatment option. It may sometimes need to be combined with grafting, or additional implants depending on the disgnosis and patient-specific factors.
Overall, atrophy can be minimised or avoided by:
- Avoidance of dentures and denture-related natural atrophy;
- Elimination of tooth-related diseases;
- Placement of implants in ideal positions and in better quality Basal bone;
- Stimulation of the bone by the presence of implants through functional use;
- Avoidance of prostheses that impair hygiene
Question 2: In essence, isn’t the removal of teeth in fact an iatrogenic cause for atrophy, an aggressive approach more specifically described as being possibly “the most destructive things that can be done to (a patient’s) jaws”.
My Reply
I think this is a very important question because it combines a question of “ethics” with the insight of experience.
PRESERVATION OF BONE
If our focus is only on preserving the bone around the teeth, then provided these are healthy or can be successfully maintained sure keeping teeth is the way to go. However, whilst this might fulfil our dominating desire (as dentists) to preserve the teeth and alveolar bone for as long as possible, this might not be acceptable to the patient.
Most of my cases are by referral, and many of those are after failed attempts and a cycle of dentistry with no clear solution to the patients issues. Here is one such letter of referral and my reply, which draw to this very point, and especially this comment by the referring dentist… “I have had a lengthy discussion …on a tooth by tooth basis and I just keep asking myself where is she going to end up despite all the well meaning efforts by the profession. I feel that continuing down the current path will eventually be doomed to failure and in the process she will have wasted considerable finances on treatment that will eventually only compromise her chances of having a more predictable and trouble-free future.”
IATROGENIC ATROPHY
Clearly the removal of teeth is an Iatrogenic cause for bone atrophy, …when the teeth are healthy. However we do not remove teeth that are healthy, or which can be saved whilst achieving an aesthetic, functional, comfortable, hygienic and desired outcome.
With respect, I don’t agree that removing unhealthy and malpositioned teeth is “one of the most destructive things that can be done to (a patient’s) jaws”. On the contrary, trying to keep them at all cost without regard to the long term outlook may lead to infections and bone destruction that can otherwise be contained with early planning. In such cases the longer we wait the less there will be to work with, the more complex (and costly) the treatment becomes, and lesser are the prospects for long term success.
From my personal experience what is far more destructive to patient’s jawbones is when implants are poorly placed or done in a way which prevents patients from being able to clean properly (see below).

There is a difference between Controlled Iatrogenic causes for bone atrophy, when we electively remove teeth and have the needed control to achieve an outcome and improve the quality of life of a patient, and Uncontrolled Iatrogenic causes when we unsuccessfully treat one problem at a time without regard to the person attached to the jaws that we are concerned about, and in doing so supervise the gradual deterioration of the dentition (supervised neglect), which is when we lose control of the outcome. To quote Robin Williams in Patch Adams “You treat a disease, you win you lose. You treat a person, I guaranty you will win no matter what”.
A terminal dentition (when teeth are still present) offers the following opportunities:
- Points of reference …which enables the surgeon to more accurately position the implants for improved aesthetics, comfort and hygiene
- Less severe bone atrophy
- Contingency
- Psycho-social impact of immediate rehabilitation
My point is that there is a difference between being Aggressive and being Definitive. The word aggressive refers to a process without any regard for the outcome. Definitive refers to the outcome, and sometimes in surgery we need to be aggressive to achieve a definitive outcome. Drawing a parallel to other areas of medicine like cancer, if this is not aggressively treated, it is not likely to succeed.
When the surgeon does not assume control of the clinical situation at surgery and adjust the bone level to allow for a hygienic tissue interface, the body will assume control and adjust it for us. Below are some other cases referred to me for revision treatment where the primary cause of bone loss was the determination to avoid being aggressive…

The above illustrates the loss of alveolar bone irrespective of the presence of implants. In the last picture the implants in Quadrant 2 (on the right of the picture) were removed and replaced with new implants in deeper basal bone. This illustrates the difference between placement of implants in alveolar bone, which limits restorative space, hampers hygiene, and does nothing to preserve bone, versus placement in basal bone which allows for improved restorative space, flat and hygienic underside, and involves a bone type that is not naturally predisposed to bundle-bone loss.

With the loss of teeth there is also a loss of opportunity to use teeth as references and correctly position the implants for improved comfort, aesthetics, hygiene and durability!

The presence of plastic flanges to overcome the shallow “conservative” placement of implants impairs hygiene and causes an inflammatory reaction and bone loss.
In the above I have offered my observations after thousands of cases, which include referrals for cases that have gone wrong when the parameters that I have mentioned are not met, many of those referred are by the very same clinicians who performed the original surgery.
Though it is a difficult decision that we all face when deciding to remove teeth, doing so early enough before losing control of the situation does present us with an opportunity to achieve a better and more stable outcome.
Question 3: We are all taught early in our careers that implants preserve the jaw bone, the hard question is: where is the evidence that (well positioned) implants do in-fact preserve jawbone?
I have dealt with this question in a separate article Do Dental Implants Help Preserve Jawbone?
The slides below are some of the relevant slides from my lectures…
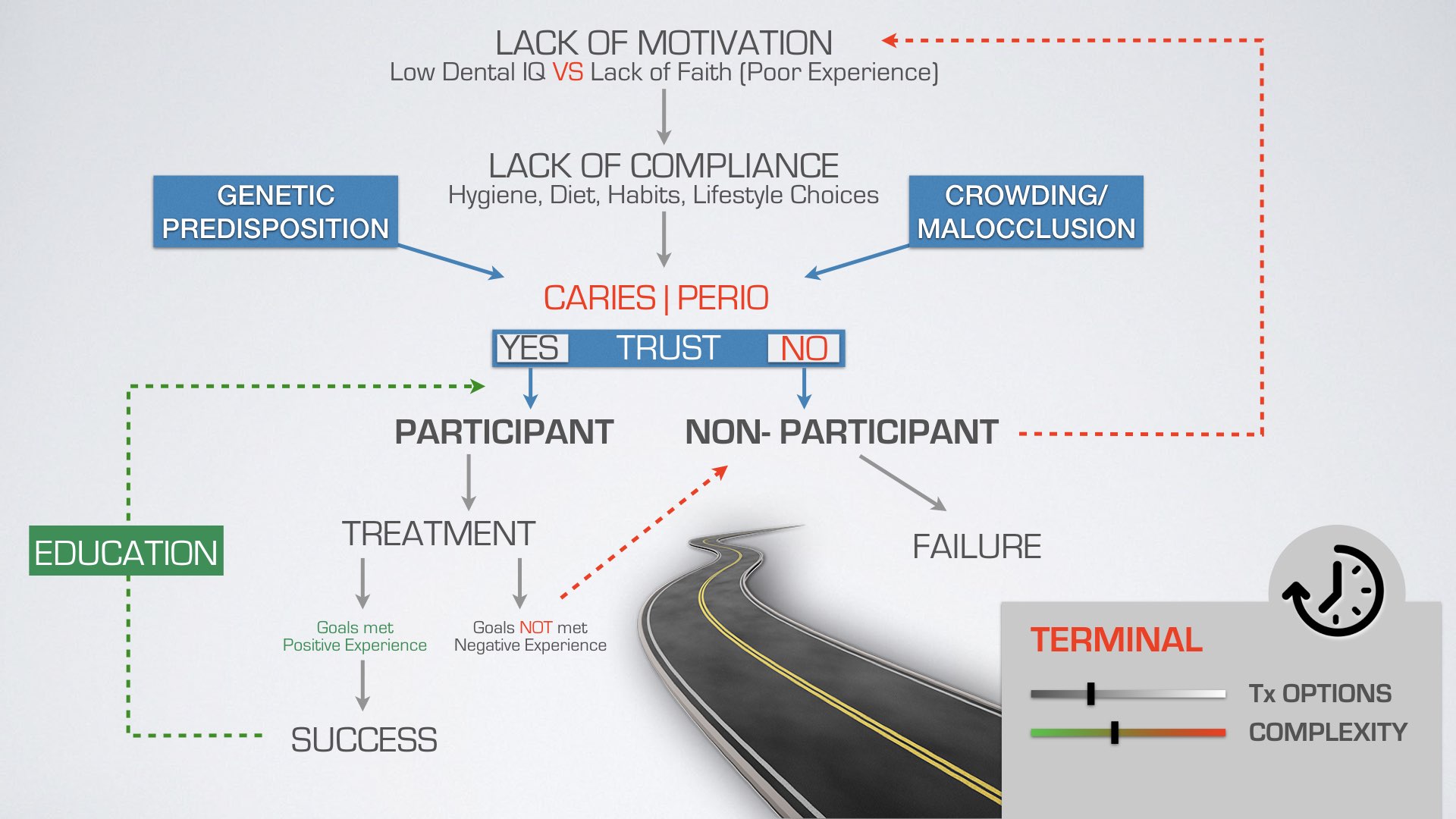
Pathways to success or failure when considering options for our patients.

A case of supervised neglect leading to severe bone loss where the case can no longer be treated with a standard All-On-4 approach. An earlier decision to remove teeth would have resulted in a simpler treatment and more predictable outcome.

The question missing here is WHEN are implants appropriate?
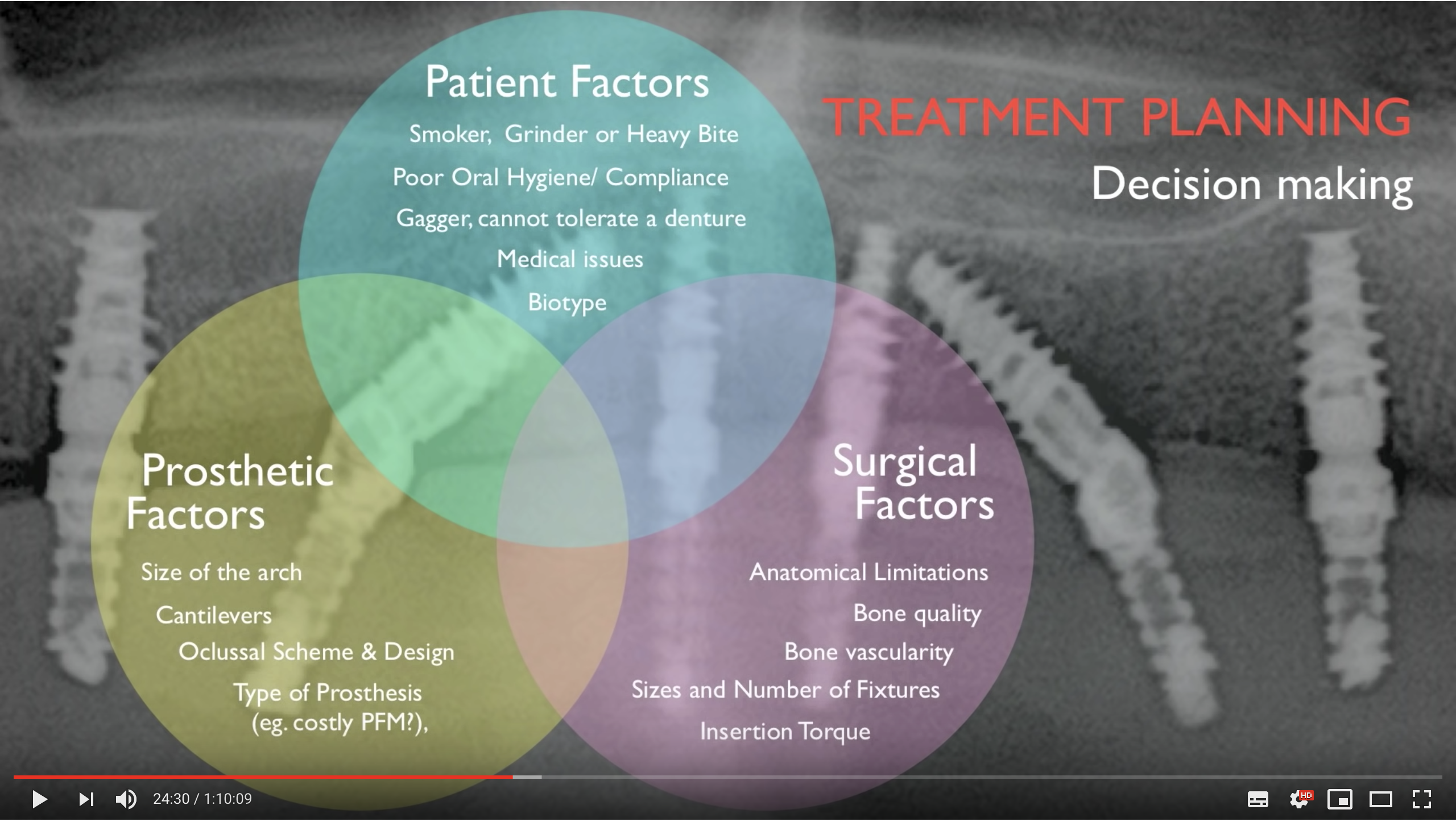
The consideration in treatment planning when deciding to keep or remove teeth are multi-faceted.

Success is very different to implant “survival”, and earlier intervention may help achieve all the required parameters for success.


