
In surgery, we often encounter situations that are not quite normal or expected, and which require adjustments (not excuses) in order to control the outcome.
The adjustments can happen before the surgery, during surgery, or when we get it wrong (if we are capable of acknowledging that this is even possible), even after surgery.
Given the individuality of our patients and differences in peri-operative conditions, adhering to a prescribed methodology or recipe may not always offer the solution we need, and thinking laterally can be key to success.
I always say if you don’t control the situation, the situation will control you. Having said that, I am conscious that regardless of our training and skills, unfortunately not every situation can be totally controlled. Tough one thing we do have an opportunity to control before we embark on any surgery is our patient's expectations, ...if we can predict or understand what those are, which does depend equally on experience/insight and planning.
In this blog series, I will explore cases where things haven't quite gone to plan, as well as cases where I made adjustments that were perhaps outside the square in order to control the outcome.
PART 1 - TRAPPED BY SPECIFIC COMPONENTS OR PROTOCOL
If we can't make the components and protocol fit the patient, make the patient fit the components and protocol?
A few days ago I saw a patient (female, late 50's) who was referred to me by a colleague and friend, with a sense of urgency in relation to the condition and state of his patient. The patient had anxiety and depression, and her current teeth appeared to make things worse. My colleague is a great surgeon himself, who is particularly sensitive to mental health issues due to his own experience and is an advocate for research and development in that branch of medicine (hence the urgency). He was perplexed by what he found and his patient's story.
The patient recently received implant treatment by an Oral & Maxillo-Facial Surgeon collaborating with a dentist, who present themselves publicly as as experts in the area of dental implants. However, in this case the outcome fell substantially short of this patient's minimal expectations.
Below is a short outline of the treatment she received.
Clinical Presentation
The patient originally presented with a full upper denture that she was unable to wear because the plastic of the denture covering her palate made her gag.
Treatment Proposal
An implant-supported fixed prosthesis was considered ideal because of the gagging from her denture.
She was told that her bone quality was very poor and that she needed quad zygomas.
Her Expectations
She expected a fixed prosthesis that does not cover the palate like her denture did, because it made her gag.
The Result
She received 2 Zygoma implants to support the bride in the back and 3 small standard implants to support the bridge in the front.


Whilst she did receive a fixed prosthesis as promised, the new implant-supported prosthesis still covers a large portion of her palate (picture 1), and is bulky and difficult to clean (picture 2).
Whereas she could choose to not wear her old denture, the current situation makes her feel trapped and helpless.
Where did it all go wrong?
This patient's Clinical Presentation is not unusual, however the fact that she was unable to tolerate coverage of her palate by her denture, and for that reason chose not to wear it, should have been a red flag.
Whilst many patients who are able to wear dentures might tolerate some palatal coverage when receiving dental implants, and in fact would often find it life-changing to have teeth that are fixed and reliable, in this case it was critical to identify the red flag and to do everything possible to minimise coverage of the palate including positioning the implants with meticulous precision according to the planned set-up and design.
After surgery the patient was told by her treating clinicians that the reason the front implants were positioned so far back into the palate was because of her bone atrophy. That may well be (and often is) the case in such situations, but if she was told of that possibility in advance she would have either declined to proceed, looked for an alternative treatment or alternative surgeons or she would have otherwise accepted the responsibility for such an outcome.
She was also told that the originally planned Quad Zygomas was not possible because the front ones would be in soft tissue.
THINKING OUTSIDE THE SQUARE
The fact that the front Zygomas would be in soft tissue is both true and not all that unusual. However whether it was, or still is, a possibility is another question altogether and requires some lateral thinking.
A quad Zygoma is often more ideal because the implants are better spread and easier to clean (provided these were positioned appropriately within the ideal prosthetic arch form). With quad Zygoma it is often the case that at least part of the anterior implant on each side is in soft tissue, this is known as extra-maxillary implants. The tips of these implants are anchored in the superior part of the cheekbone, or the inferior/lateral orbital rim so anchorage/support for the bridge are highly reliable. Though it is a fact that the more ideal within the arch form we want the emergence of the implants to be, the more extra-maxillary part of the shaft will become. So what is the problem with that?
Whilst the technique is complex and there are some minor risks at the insertion point (not dissimilar to other Zygoma techniques), the main concern is tissue dehiscence and exposure of the implant. However, if we turn this from being a concern to an expectation, we can improve the outcome by using some bone grafting to fill any surgical dead space between the implant and lateral aspect of the maxilla, and importantly by using an implant that has a polished collar to facilitate hygiene once recession of the expected tissue occurs.
We could also consider some soft tissue management to improve the biostability.
What can be done?
Revision surgery is complicated not only technically but also philosophically. The patient has invested significant money and the surgeon/dentist have expended much of their own efforts to provide the treatment to the best of their abilities.
Here are the options:
Option 1 – do nothing else surgical, and make adjustments to the existing bridge to reduce the thickness, possibly even consider a thin metal plate without the acrylic coverage. This will reduce the thickness but not the positions of the implants. This is not something this patient is willing to accept because her issue is with the palatal position not just the thickness. Nonetheless, it is worth a try considering the alternatives have more risks.
Option 2 – decommission and burry all the implants, and go back to having no teeth (since a denture is not an option). The patient feels she has gone through so much already and would like to avoid going back to square 1. She is willing to try anything possible irrespective of the risk to reposition the front implants.
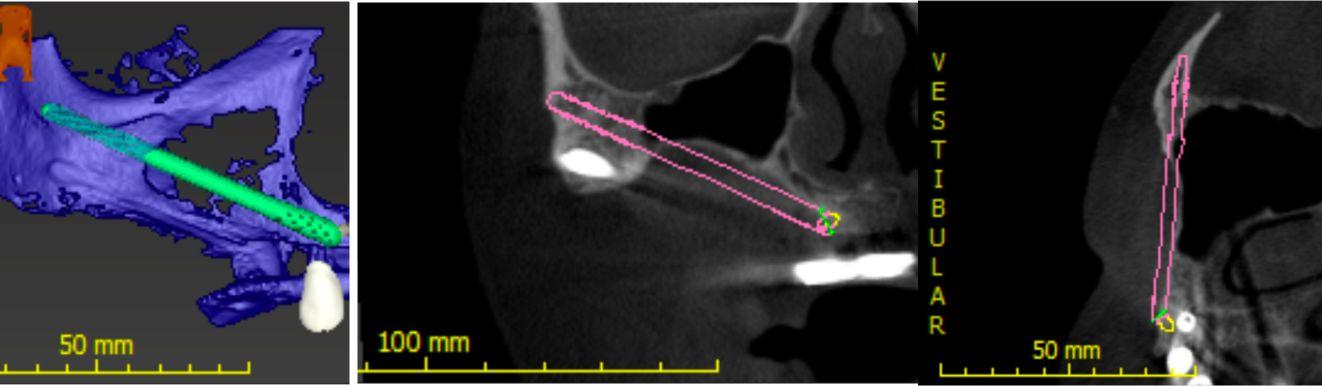
Option 3 (Beyond the Square) – accept the posterior Zygoma implants, and decommission and bury the front implants and reconsider the original plan for Quad Zygomas by placing the anterior Zygoma implants using the above extra-maxillary method. Considering the extreme palatal positions of the existing anterior implants this is likely to be possible without even removing them, which also has an element of contingency where she could always go back to what she has now. The pictures below shows the 3-d trajectory of the anterior Zygoma implant without removing the existing front implants.
The most complex part of this revision (at least if I was doing it) would actually be managing the soft tissues. As a result of the prior surgery and holes in the keratinised mucosa from the prior implants there is less tissue to work with, but split-layer pedicle grafts and healing through secondary intention should be considered nonetheless. In any event, the patient’s expectations will need to be adjusted accordingly, in particular the fact that there is a moderate chance despite our best efforts that tissues surrounding the implants would be of a thin nature and sensitive to brushing. A small space may need to be created to facilitate cleaning, which may allow air to escape potentially affecting speech.
Whilst it would be ideal to also replace the posterior Zygoma implants for better emergence within the arch, their removal once integrated is complex and can destroy the opportunity to insert a replacement implant. This is also not the core of the complaint, thus it is an unnecessary risk.
What about other options?
Angulated Abutments – these were already used on the existing implants. Even if further correction was achievable, the base position of the front implants would not change, which is the root of the problem.
Overdenture – An overdenture will require clips and components within it to attach to the implants, and would be far bulkier than the fixed bridge. Considering the palatal positions of the existing front implants, this is likely to be far worse for this patient.
What Now?
This patient comes across as sad and lost, not only in relation to where she is at with her teeth, but also in what she felt was a dismissive attitude by her providers and their poor communication.
I was unable to reconcile the philosophical and ethical constructs of this case and I referred the patient back to her surgeon and dentist. I have written to them privately encouraging them to explore the above options with their patient.


